<< Back
Here’s a Roadmap to Skin Cancer . . . And a Way Out

September 28, 2021
By Dr. Dean David George
Medical Director, Cutaneous Oncology
Hartford Healthcare Cancer Institute
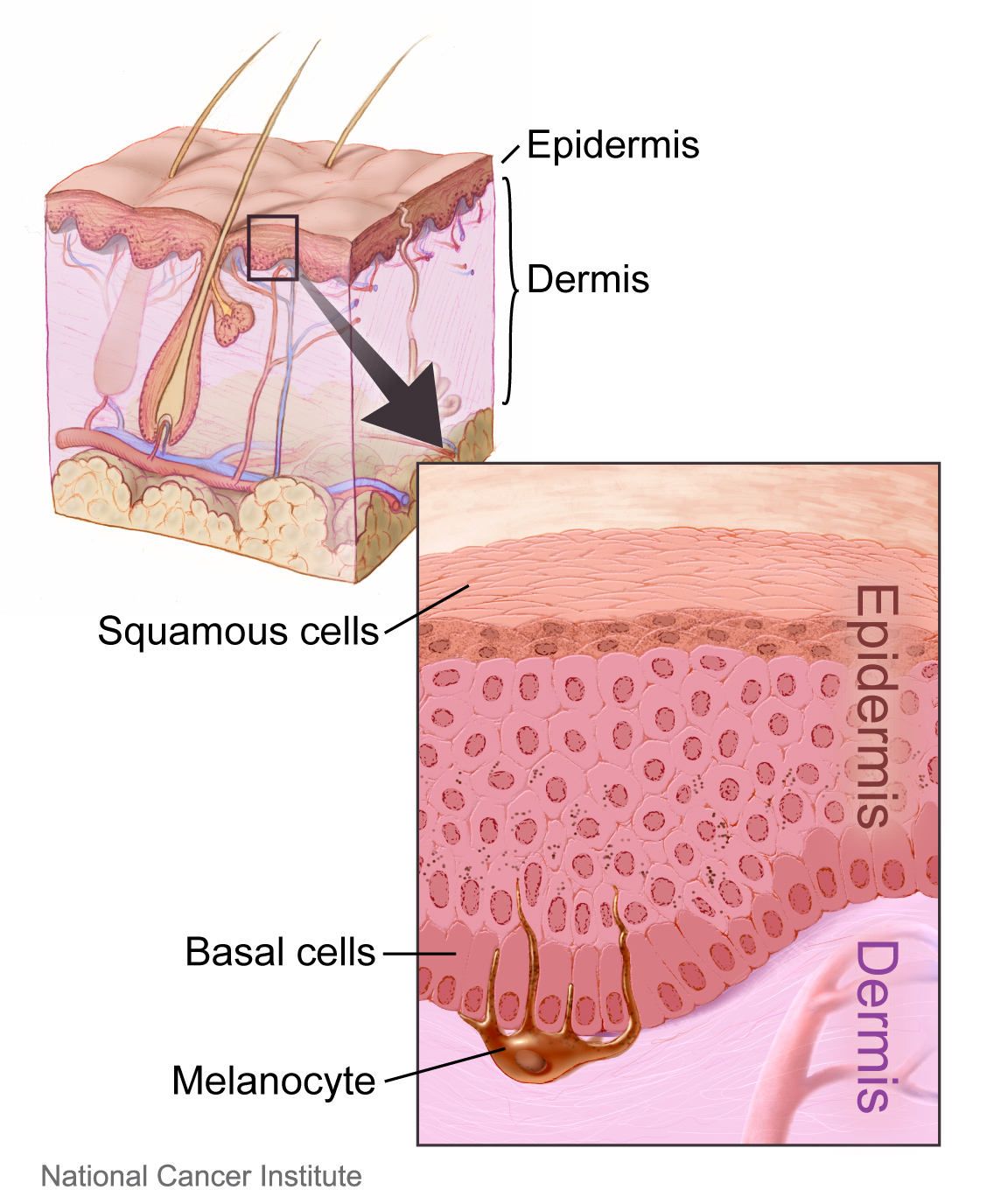
Your skin is composed of three layers: the epidermis, dermis, and subcutaneous fat.
The epidermis is the part of your skin that renews itself roughly every 28 days. The living cells here are called keratinocytes because they produce keratin, the protein the makes the outermost part of your skin resistant to the external environment.
The dermis appears white and is composed mainly of the proteins collagen and elastin which give your skin its strength. Blood vessels, nerves, sweat glands, and hair follicles can be found here.
The subcutaneous layer is where your fat cells reside, providing insulation and cushioning for your skin.
The epidermis is composed of five layers from outside to inside: the stratum corneum, stratum lucidem, stratum granulosum, stratum spinosum and stratum basale. The stratum lucidem is only found on the palms and soles giving these areas extra strength. Cube-shaped basal cells on the stratum basale are interspersed with melanocytes, the cells that produce pigment.
Basal cells give rise to squamous cells, which flatten and fill with keratin as they go through their 14-day life cycle transitioning to corneocytes. The dead corneocytes then take another 14 days to flake off and become part of the dust in your house. Think of the outermost layer of your skin as a paved stone road where the stones are corneocytes and the mortar is the substance they secrete while filling with keratin.
Keratinocyte cancer encompasses both basal (approximately 75 percent) and squamous cell carcinomas (approximately 25 percent). It is the most common skin cancer in the United States, affecting men more than women with a sharp increase over age 60. Skin type and lifetime ultraviolet light exposure are the major risk factors.
Basal cell carcinoma occurs when basal cells make more copies of themselves instead of squamous cells. Squamous cell carcinoma occurs when squamous cells make more copies of themselves instead of becoming corneocytes. Both types of cancer do not frequently metastasize (spread to other parts of the body), especially when caught early.
Your doctor will perform a skin biopsy of a suspicious lesion to look at under the microscope to determine if it is cancer. If the cancer is contained in the epidermis, it may be amenable to treatment with topical chemotherapy cream, scraping & burning, or liquid nitrogen. If it has moved into the dermis, it will likely need to be removed with a minor outpatient procedure under local anesthesia.
When it comes to skin cancer, an ounce of prevention really is worth a pound of cure. Apply broad spectrum SPF 30 or greater sunscreen to exposed skin when outdoors and wear wide-brimmed hats, sunglasses and sun shirts. Avoid tanning beds, sun lamps, and tanning salons.
Seek shade whenever possible. Be sure to check your skin monthly. Use a ruler to measure and smartphone to photograph any suspicious lesion and monitor them. Tell your doctor right away if you find a lesion that is changing, growing, itching or bleeding so it can be properly evaluated by a board-certified dermatologist.
If you are high risk due to prior skin cancer or if you are immunocompromised, you might benefit from an annual total skin exam by your dermatologist.