<< Back
NFL Week 14 Injury Report: How a Torn Meniscus Can Change Your Life
December 05, 2017
Our weekly NFL report evaluates injuries to players of local (Patriots, Giants and Jets) or national interest with commentary by a sports orthopedic specialist from the Bone & Joint Institute at Hartford Hospital. Sign up for automatic delivery to your inbox (click here and scroll to “Free email newsletters”).
Player: Kelvin Benjamin, Buffalo Bills wide receiver.
Injury: Torn meniscus (left knee).
How it happened: Benjamin fell awkwardly when tackled after a 20-yard pass play on the opening possession of the Bills’ 54-24 loss Nov. 12 to the Los Angeles Chargers.
Expected time missed: A torn meniscus should not end an NFL player’s season — as long as the season doesn’t end before the 4-6 weeks it takes to recover from this injury. The Bills initially classified Benjamin as day-to-day. That diagnosis proved optimistic. Benjamin tore the anterior cruciate ligament in the same knee while with the Carolina Panthers in 2015 during a joint practice with the Miami Dolphins. His latest injury could raise concerns about his longevity in the NFL.
Dr. Clifford Rios, Bone & Joint Institute orthopedic surgeon and board-certified in sports medicine: “A partial meniscectomy for a tear that involves relatively little of the meniscus will allow a quick return to sport. A repair of any significance will keep someone out 4-5 months, at least. Most athletes are going to be treated surgically. If the tear is small, they can try to get through the season on it, particularly if there are not many symptoms.
“The risk is another injury causing a larger tear. Meniscectomy in an NFL lineman, for example, is more detrimental to knee function and career length than an ACL injury. That’s likely because meniscus is a critical shock absorber and in heavier people degenerative arthritis will occur rapidly after loss of meniscus. In Benjamin’s case, the overall outlook on his career is not good. For reasons above, plus the extreme load that NFL players put on their knees, I suspect his knee function will deteriorate rapidly over the next few years.”
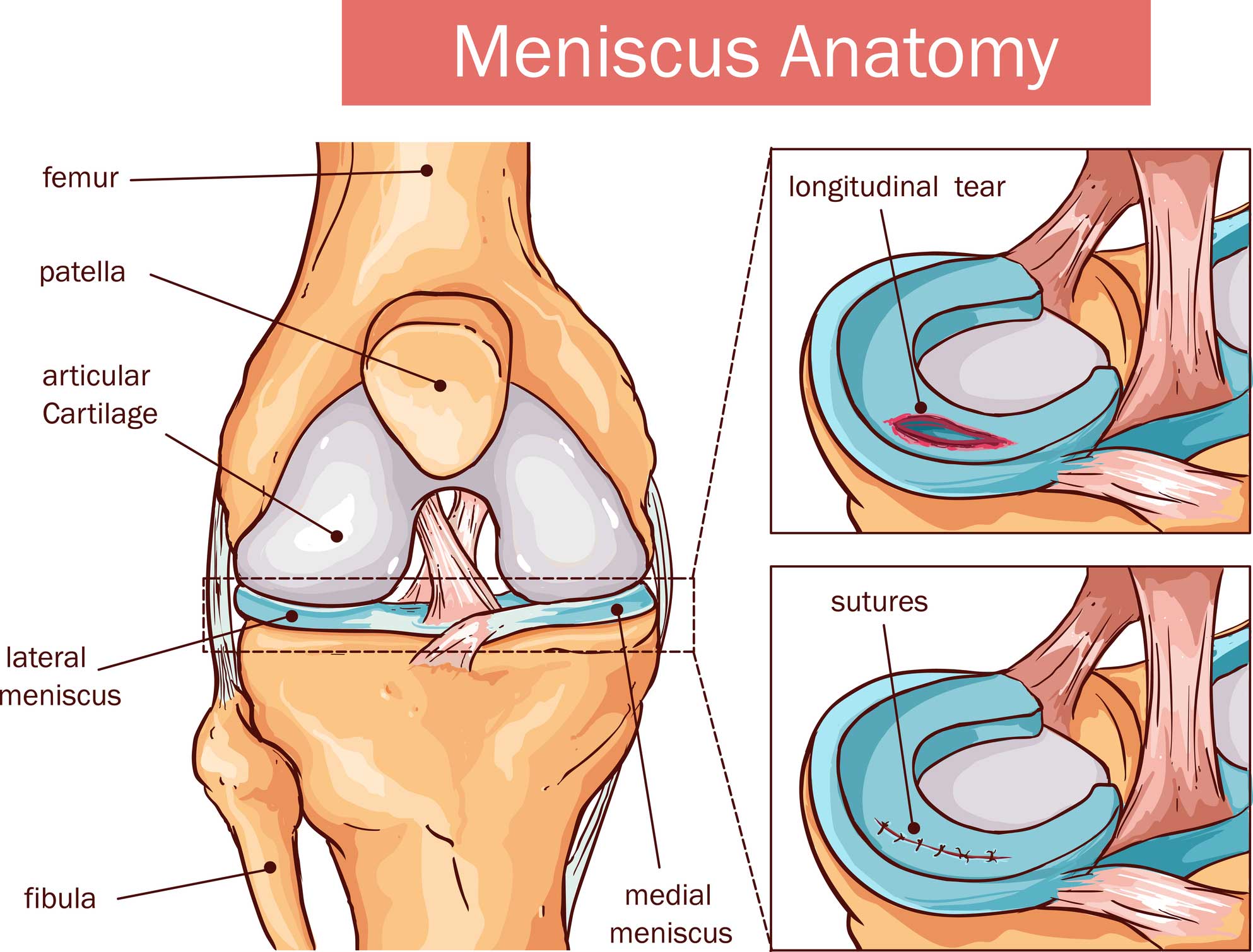
What is meniscus?: It’s rubbery, C-shaped cartilage in your knee joint that acts as a shock absorber between bones in a joint. The knee includes the thigh bone (femur), leg bone (tibia) and kneecap (patella). Each knee, between the femur and tibia, has an inside (medial) and outside (lateral) meniscus.
The risks: A blow to the knee, like a hard tackle, can causes a tear. Twisting or overextending your knee and quick direction changes can cause a meniscus tear, too. In everyday life, squatting to pick up a coin on the ground can do it.
First signs of torn meniscus: Pain, on either side of the knee (not around the kneecap), and swelling. An athlete often describes the sensation of tearing a meniscus as a pop. Running back Adrian Peterson, then with the Minnesota Vikings, suffered a torn meniscus in Week 2 in 2016 and required lateral surgery. He played only one more game (Week 15) before his season ended because of knee and groin injuries.
Recovery/Treatment: First, your doctor will want an MRI to see if the meniscus has been stretched or torn and X-rays that will reveal any damage to the surrounding bones in the knee. If it’s a mild tear, some RICE will help:
- Resting your leg.
- Icing your knee three or four times a day for 20 minutes.
- Compressing the affected area with a compression wrap or elastic bandage.
- Elevating your leg above heart level.
Surgery: If surgery is required, your doctor will repair or trim the meniscus using an arthroscope. In most cases, the torn fragments are removed. About 80 percent of the meniscus has no blood supply, which prevents healing when torn (even after being repaired and stitched). Recovery is longer for a repair, but preserves the knee’s long-term function.
“The meniscus does not heal on its own without surgery,” says Dr. Rios. “Some people can have tears and have minimal or no symptoms, but that does not mean that it healed. I suspect if Benjamin’s tear were in the peripheral third, where the blood supply is, someone would advocate fixing it before it gets worse and possibly becomes irreparable. If the tear is in the avascular area, he can try to play and, worst case, do a partial meniscectomy if symptomatic.
Removing torn meniscus, a minimally invasive procedure, requires two or three small punctures. The patient might need crutches for a few days, but the non-athlete can return to work in a couple days. The athlete can return in 4 to 6 weeks, which includes physical therapy.
Meniscus removal, for any patient, increases the risk of arthritis starting at age 45 to 50.
“It’s very high,” says Dr. Rios. “I had my lateral meniscus removed 20 years ago and I weigh 180 pounds. I already have arthritis and cannot run. Degenerative joint disease is present on nearly all radiographs 10 years after meniscectomy, but in these heavier athletes with high stress on the knee I would expect arthritic changes much sooner, likely within five years. The extent of arthritis depends on amount of meniscus tissue that is lost. In general, I advise my patients after a mensicectomy to give up distance running and chose lower-impact cardio for just this reason.”
Dr. Clifford Rios, a sports medicine surgeon with Orthopedic Associates of Hartford, is Site Director for orthopedic resident education at the Bone & Joint Institute. Click here to find out why the Bone & Joint Institute is the athlete’s choice, with a Motion Lab for performance analysis, the area’s most comprehensive sports rehabilitation facility and 30 fellowship-trained orthopedic surgeons.